
CMS-0057-F is the U.S. Centers for Medicare & Medicaid Services (CMS) Interoperability and Prior Authorization Final Rule. It applies to selected U.S. health plans that work with federal programs, including Medicaid and CHIP agencies, Medicaid managed care plans, CHIP managed care entities, and QHP issuers on the federal exchanges.
The rule pushes these payers to move from basic data sharing to automated prior authorization decisions, FHIR® APIs, and public reporting of performance metrics.
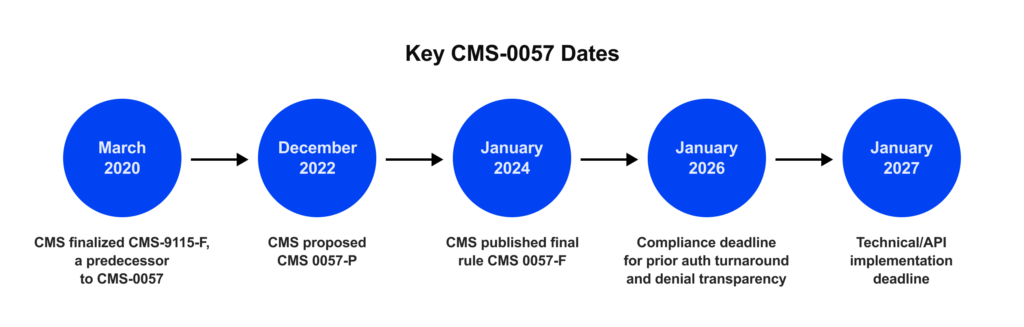
If you run a health plan, a third-party administrator (TPA), or provide revenue-cycle management solutions, CMS-0057-F is the next big deadline. It moves the market from basic data sharing to automated decisions and public metrics. Practically, that means Patient, Provider, Payer-to-Payer, and Prior Authorization FHIR APIs by January 1, 2027; faster prior-auth turnarounds start January 1, 2026, and the first public PA metrics are due March 31, 2026.
Centers for Medicare & Medicaid Services (CMS), the U.S. federal agency within the Department of Health and Human Services that administers Medicare, expects approximately $15 billion in savings over 10 years as prior authorization goes digital. CAQH shows ~14 minutes saved per authorization and $515M in annual industry savings with electronic standards.
Yet physicians still handle ~43 prior authorizations (PAs) per week and spend ~12 hours on them—pressure that spills back into your network experience. Learn more about the FHIR prior authorization automation and AI for prior authorization in our recent articles.
This guide explains the CMS rule in plain language and outlines practical options for implementation. You’ll learn the practical requirements, possible challenges, and practical roadmap. Learn more about our HL7 FHIR services to explore all cooperation opportunities.
Highlights:
- CMS-0057-F moves payers from data sharing to automated decisions with FHIR APIs and public metrics.
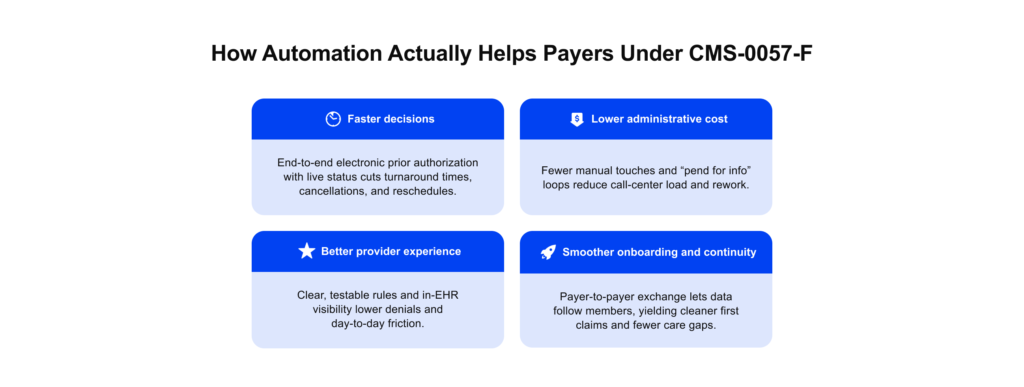
- Expected impact is faster decisions, fewer manual touches, cleaner claims, and measurable transparency.
- Benchmarks show about $15B in savings projected by CMS over 10 years, about 14 minutes saved per request per CAQH, physicians still average about 43 PAs a week and about 12 hours on them.
What is the CMS-0057-F Interoperability Rule?
The CMS-0057-F, formally the CMS Interoperability and Prior Authorization Final Rule, updates the 2020 CMS Patient Access rule and moves the market from simple data access to standardized, automated exchange using CMS FHIR APIs. A FHIR API is a standards-based web interface built on HL7 FHIR (Fast Healthcare Interoperability Resources).
FHIR defines common data models and REST patterns for health information, enabling payers, providers, and apps to exchange claims, clinical data, and prior-authorization details in a consistent, machine-readable manner, rather than relying on custom, one-off integrations.
It adds three payer APIs (Provider Access, Payer-to-Payer, Prior Authorization (PA)) and strengthens the CMS interoperability and Patient Access API, with firm timelines and public reporting.
The CMS interoperability rule aims to reduce delays, enhance data exchange, and increase transparency across payers and providers.
In short, CMS-0057-F turns interoperability into day-to-day automation that reduces delays and lowers administrative burden across plans and providers. CMS wants U.S. healthcare to run on shared, digital rails. The goal is simple: faster decisions, less paperwork, and a better experience for members and providers. CMS-0057-F pushes the market from “share the data” to “automate the process” using open FHIR standards inside everyday workflows.
Strategically, CMS is moving in stages: first access, then exchange, and now automation. Coverage and documentation rules become rules as code, so systems can check requirements and return decisions automatically. Public metrics make performance visible, and patient control ensures data follows people across plans without delays.
Notably, the rule aligns with the HL7 Da Vinci Project, but Da Vinci is not the only way to comply. CMS does not mandate FHIR-based backends or Da Vinci implementation guides; any architecture that delivers the required data and functions can meet the rule.
In practice, Da Vinci has become the preferred playbook because it turns policy language into concrete, testable FHIR workflows that EHR vendors and payers already understand. The project publishes detailed implementation guides, example payloads, and conformance expectations, which reduces ambiguity and shortens integration cycles.
For prior authorization, Coverage Requirements Discovery (CRD) checks if PA is required, Documentation Templates and Rules (DTR) collects the exact evidence, and Prior Authorization Support (PAS) submits and tracks requests directly inside EHRs.
CMS-0057-F requires a FHIR Prior Authorization API and points to these Da Vinci guides as the preferred path; they aren’t strictly mandatory yet, but CMS clearly signals that direction. HHS also allows an all-FHIR PA flow instead of X12 278 under enforcement discretion, so using Da Vinci helps you comply faster and integrate cleanly with provider systems.
Why this matters: Prior authorization involves multiple stakeholders, including payers, providers, TPAs, and sometimes pharmacies. Without shared, open standards, the handoffs break. Da Vinci brings a familiar playbook that supports coordinated, value-based care and the automation CMS expects.
Operational improvements (faster PA decisions and metric collection) start January 1, 2026. Required FHIR application programming interfaces (APIs) must be live by January 1, 2027.
Planning milestones for payers:
- January 1, 2026: Faster PA decision timelines begin; metric collection starts.
- March 31, 2026: First public PA performance metrics are due.
- January 1, 2027: Patient Access, Provider Access, Payer-to-Payer, and PA APIs must run in production (managed-care programs align to rating periods).
With CMS-0057-F deadlines approaching, many payers require a partner that can translate regulatory language into functional platforms, APIs, and operational systems.
Edenlab is a healthcare IT partner company focused on data exchange regulatory compliance and health operations automation. We design and implement FHIR-based systems that map legacy data, align with CMS, embed privacy and auditability, and implement Da Vinci where it fits. So prior authorization, claims, and member services run smoothly.
Recently, we designed a revenue-cycle data platform that acts as a message-exchange hub between providers and payers. It supports eligibility checks, prior authorization, claims, remittances, and payment reconciliation using a FHIR Messaging approach, creating end-to-end visibility, faster adjudication, and fewer exceptions across the network.
To move fast, we use FHIR-native accelerators, such as our Kodjin Data Platform, for repository, terminology, and SMART on FHIR. Kodjin speeds delivery but isn’t a stand-alone Da Vinci solution; when needs extend beyond it, we bridge with custom services, partner components, and your stack to meet CMS-0057-F on time.

Key CMS-0057-F Interoperability Requirements
CMS-0057-F gives impacted payers two hard dates: new prior authorization (PA) turnaround rules from January 1, 2026, and production-grade APIs live by January 1, 2027.
All of these APIs are defined as HL7 FHIR APIs. FHIR is the main modern standard for structuring and exchanging health data over REST APIs, but it does not mean every internal system must become FHIR-native on day one.
Below, we explain each API in plain language and why it matters.
Patient Access API
The Patient Access API enables members to view their claims, encounters, clinical data, and prior authorization information for items and services (excluding drugs) through an app of their choice. Members should be able to check status, dates, and the reason a request was approved or denied, regardless of how the request was submitted.
Under CMS-0057-F, payers must also track the number of unique members using this API and the frequency of their use, and report these metrics to CMS. In practice, this API becomes the main way for both members and regulators to see whether digital access is actually working.
Provider Access API
The Provider Access API provides member data to in-network providers with a treatment relationship to the patient. It exposes claims and encounter data (excluding remittances and cost-sharing), clinical data, and selected prior authorization details, allowing clinicians to prepare care and view PA status within their EHR workflow.
Payers must maintain an attribution process to determine which providers can access which members’ data, support patient opt-out, and provide plain-language explanations of what is shared. When implemented well, this API replaces portal hunting and phone calls with data that lands directly in point-of-care systems.
Payer-to-Payer Data Exchange
The Payer-to-Payer API supports continuity when members move between plans. With member opt-in, the new plan can request up to five years of claims and encounter data, clinical data, and relevant prior authorization information from the prior or concurrent plan over a secure FHIR API.
Financial information such as remittances and cost-sharing is excluded. For concurrent coverage, data should be refreshed on a regular schedule, so both plans work from a consistent record instead of rebuilding history from scratch.
Prior Authorization API
Publish a computable catalog of covered items/services and required documentation, accept electronic requests, and return structured outcomes, approve (with dates/conditions), deny (with a specific reason), or request more information. Meet decision SLAs (urgent vs. standard), surface status changes in real time, and generate public performance metrics.
| How it works in practice | |
| Coverage discovery (CRD) | At order time, the EHR checks whether PA is needed for this member, service, and setting. |
| Documentation automation (DTR) | The system returns an exact Questionnaire of evidence (labs, notes, imaging) and auto-collects what already exists. |
| Submission & tracking (PAS) | The request goes in electronically (FHIR Claim/ClaimResponse with optional X12 278 bridge) and updates flow back via Subscriptions/webhooks. |
| Denial transparency | Machine-readable denial reasons let teams fix issues quickly and fuel appeals and quality programs. |
| Reporting | Timeliness, volume, and outcomes roll up to dashboards and the public posting CMS requires. |

CRD/DTR/PAS are the preferred FHIR playbooks for this API. They aren’t strictly mandatory today, but they deliver the end-to-end automation that the CMS expects and integrate cleanly with EHRs, making them the fastest and least ambiguous path to compliance.
Waiting until March 2026 to act leaves little time to redesign workflows, clean data, and integrate with provider systems. Compliance gaps can trigger CMS scrutiny and public metrics that are hard to improve after the fact.
Manual exceptions then pile up, driving up cost-to-serve and frustrating providers and employer groups. The pragmatic approach is to modernize once and reuse the same standards-aligned core across products and lines of business, instead of building one-off fixes for each program.
Need expert assistance with regulatory compliance?
We are here to help. Check our
Healthcare regulatory compliance servicesWhy the Rule Matters for Payers
For health plans and TPAs, this rule reshapes day-to-day operations. Your APIs become the front door for providers and members, and automated decisions start to define service quality, operating cost, and satisfaction. When data moves smoothly and decisions are made quickly, contact centers shrink, rework decreases, and provider relationships become easier rather than more complicated.
| Business process | APIs / Guides | What happens (flow) | Business impact |
| Pre-visit coverage | Provider Access API; CRD | At order entry, the EHR calls CRD; your rules return whether PA is required for this member, service, and setting; the result is shown in-workflow. | Fewer no-auth denials and cancellations; tighter schedules; higher provider satisfaction. |
| Evidence collection | Provider Access API; DTR | DTR returns an exact Questionnaire; system pulls existing labs/notes/imaging and pre-fills required fields for review and submits. | Lower pend rates; shorter cycle time; less staff time chasing documents. |
| Electronic submission | Prior Authorization API; PAS; FHIR Subscriptions | The EHR submits a structured PA; status changes (pend/approve/deny) auto-notify systems and staff; denial includes a specific reason. | Faster determinations; fewer status calls; higher first-pass approvals; clean audit trails. |
| Discharge planning and post-acute coordination | Provider Access API; CRD/DTR for DME/Home Health | Hospital checks benefits and PA needs pre-discharge; orders include current coverage and documentation; updates flow to care teams. | Smoother transitions; fewer avoidable readmissions; better member experience. |
| Claims pre-population and auto-adjudication | Prior Authorization API; PAS IDs on claim | Approved auth IDs and conditions flow into the claim; rules engine validates policy/benefits before adjudication. | Higher first-pass payment; fewer reworks/appeals; lower cost-to-serve. |
| New-member onboarding and plan switches | Payer-to-Payer API (opt-in) | New plan imports up to five years of claims/clinical/PA context from prior plan; for concurrent coverage, refresh on a schedule. | Faster onboarding; safer care continuity; better risk capture and quality scores. |
| Provider pre-visit preparation | Provider Access API; (optionally) Bulk FHIR | Practices pull history and open PA context before visits; tasks/tests visible in one place for team action. | Fewer duplicate tests; higher visit quality; improved Stars/HEDIS results. |
| Member self-service | Patient Access API; SMART on FHIR | Member app shows benefits, claims history, PA status; secure login/tokens managed via SMART/OIDC. | Lower call volume; better CAHPS; stronger retention with employer groups. |
| Appeals and grievances automation | PAS denial reasons; DTR; DocumentReference | Machine-readable denial reasons trigger templated outreach; system assembles exact evidence for appeal submission. | Faster resolutions; fewer missed deadlines; reduced compliance risk. |
| Network performance | All four APIs; orchestration metrics; public posting | API layer captures timeliness/volume/outcomes; dashboards reconcile with machine-readable public reports. | Transparent performance; stronger vendor governance; clearer employer reporting/renewals. |
Modernization delivers compounding benefits. Consistent data flows reduce exceptions, shorten revenue cycles, and make onboarding less painful for employer groups. Clear, testable rules improve authorization quality and cut back-and-forth. Transparent performance, uptime, timeliness, and accuracy, builds trust with regulators and the market.
Product Opportunities Under CMS-0057-F
Edenlab partners with product teams to turn regulatory change into shipped features. We co-design and co-build payer-grade connectivity, automation, and compliance tooling, bringing FHIR-native accelerators (including our Kodjin platform) when they speed things up, and integrating cleanly with your existing stack.
Product opportunities to build now
- Claims and utilization modernization. Make claims prior-auth–aware (link authorization IDs and conditions), emit specific denial reasons, and keep end-to-end audit trails.
- FHIR-first connectivity. Software kits and adapters for all four required APIs (Patient, Provider, Payer-to-Payer, Prior Authorization), plus electronic health record components such as SMART on FHIR apps and real-time subscriptions.
- Rules as code. Policy authoring, versioning, and automated tests so coverage and documentation rules can change safely and predictably.
- Prior-authorization gateways. Prior Authorization Support services for electronic submit/status, with optional X12 278 bridges where Electronic Data Interchange (EDI) remains.
- Metrics and public reporting. Pipelines that generate CMS-ready, machine-readable files and reconcile them with internal dashboards.
- Sandboxes and simulators. Provider-friendly test environments that shorten onboarding and reduce integration risk. Learn more about our healthcare integration solutions.
Meeting the rule starts with a clear foundation: a single, secure FHIR gateway that enforces access, captures consent, and logs every action. Encode coverage and documentation as executable rules, and test policy changes like code. Automatically push status updates into EHRs and portals. Monitor performance, set SLAs, and scale for peaks so service stays reliable.
Implementation Challenges and How to Overcome Them
Teams often hit the same blockers when turning CMS interoperability policy into working systems. The list below pairs each challenge with technical and organizational moves that work under healthcare interoperability CMS mandates.
- Legacy tech and old formats. Some partners still use EDI/X12 and lack modern APIs. Modern FHIR APIs can be bridged to older formats, with short-lived automation treated as a temporary measure with a clear sunset.
- Access and consent. Payers must control who sees what and capture member opt-in/opt-out clearly. Robust access-control patterns enforce permissions, record consent decisions, and maintain an auditable trail for every access event.
- Prior-auth rules keep changing. Static PDFs and manual updates cause errors and rework. Turning policies into versioned, testable rules allows safer rollouts, easier regression testing, and predictable updates.
- No visibility in the clinician’s workflow. If status is not visible inside the EHR, adoption stalls. Guidance and real-time updates should appear directly in the chart, removing calls, emails, and portal hunting.
- Peaks and scale. Renewals and program changes create traffic spikes. Architectures designed for surge capacity, with clear reliability targets, keep service steady under load.
- Public metrics and audits. Manual reporting invites errors and audit findings. Metrics collected at the source can feed machine-readable reports and immutable audit logs, reducing preparation time and compliance risk.
- Multi-team delivery slows down without clear ownership. Cross-functional work drifts when no one owns outcomes. A single delivery plan with shared decisions, explicitly owned interfaces, and agreed error handling keeps releases on track.
- Timelines slip when the scope is huge. Trying to build everything at once delays value. A thin end-to-end slice, proven in production and then expanded line by line, helps hit the 2026/2027 milestones.
These risks shrink when the partner has done it before. At Edenlab, we’ve implemented FHIR in some of the world’s largest interoperability programs. A recent example is our work with Elation Health in the U.S.
We built a FHIR-compliant backend that bridged their existing EHR to 21st Century Cures Act API standards, helping them achieve ONC certification without a ground-up redesign. Using a custom clinical-data mapper on the Kodjin FHIR Server, we delivered seamless interoperability, strong performance, and full SMART on FHIR support.
Read also:
Strategies for Overcoming Interoperability Challenges in Medium Healthcare Organizations
Read the case studyWhy Edenlab Is Your Reliable Partner in AI Prior-Authorization Automation
Edenlab focuses solely on healthcare. We pair IT consulting and deep business analysis with data engineering and hands-on claims expertise. We design AI-ready data foundations and build FHIR-first, audit-ready workflows with privacy and governance from day one.
We translate CMS-0057-F from policy to production. Our teams deliver Patient, Provider, Payer-to-Payer, and Prior Authorization APIs, implement Da Vinci, and encode benefit rules as executable logic. We wire consent, identity, and telemetry into the platform and produce the metrics and evidence you must publish.
We integrate cleanly across your ecosystem. EHRs connect via FHIR or HL7v2. Payer APIs, clearinghouses, and claims cores align through stable interfaces. We deploy on AWS, Azure, or GCP. Under the hood, we utilize NLP and ML for evidence extraction and denial prediction, RPA to overcome legacy portal limitations, event streaming for real-time status updates, rules engines for determinations, MDM for member/provider identity management, and full observability.
The results are tangible. Routine requests move in hours, not days. First-pass approvals rise. Resubmissions and manual touches fall. Administrative cost per request drops. Audit trails stay clear, consistent, and ready for review.
We also proved the pattern at practice. Recently, we’ve partnered with Heals.Asia, one of Hong Kong’s largest TPAs. By implementing a FHIR-based auto-adjudication engine that evaluates claims and pre-authorizations against complex plan rules, deductibles, co-pays, and more, decisions arrive faster, manual work drops, and the solution fits existing business processes without disruption.
Conclusion
CMS-0057-F is a move from sharing data to automating decisions in everyday workflows. When implemented well, plans see faster determinations, fewer manual steps, cleaner claims, and a more transparent experience for members and providers. The timelines are set; the opportunity is to use them to modernize in a practical, measurable way.
A sensible approach is to select a standards-aligned foundation, demonstrate one high-value workflow end-to-end (for example, Provider Access with prior authorization status within the EHR), and scale from there. Instrument the flow with clear metrics, involve provider partners early, and use Da Vinci where it fits to keep integrations predictable. This enables regulatory work to be leveraged as a reusable capability across lines of business.
Edenlab can help you make that transition. We deliver regulation-aligned CMS payer-to-payer data exchange and healthcare automation services, and we bring FHIR-native accelerators, such as our Kodjin platform, to shorten delivery when appropriate. If you’re planning for the 2026/2027 milestones, we’re ready to map your readiness, select the first workflow to prove, and build a roadmap you can execute with confidence.

Ready for 2026/2027
From Patient, Provider, and Payer-to-Payer to Prior Auth, we deliver standards-aligned workflows that providers actually use.
FAQs
What is the CMS-0057-F interoperability rule?
It’s the CMS Interoperability and Prior Authorization Final Rule. It moves payers from basic data sharing to FHIR-based APIs and automated decisions, especially for prior auth. The goal: faster care decisions, lower admin cost, and a better experience.
Who needs to comply with CMS-0057-F?
Medicare Advantage plans, Medicaid and CHIP (FFS and managed care), and QHP issuers on the Federally-facilitated Exchanges. TPAs and vendors must support these capabilities when they operate for impacted plans.
What are the CMS interoperability requirements for payers?
Stand up four APIs, Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization, with strong security and consent. Provide machine-readable denial reasons, meet faster decision timelines, publish adoption and timeliness metrics, and educate members about data sharing.
How can automation help meet CMS-0057-F compliance?
Use API orchestration and the Da Vinci playbooks (CRD, DTR, PAS) to drive in-EHR checks, auto-gather documentation, submit requests electronically, and push real-time status updates. Tie determinations to claims and eligibility. Automate metrics and audit trails. The result: fewer touches and shorter cycle times.
What is the deadline for CMS-0057-F implementation?
For CMS-0057-F, the clock runs in three steps: starting January 1, 2026, faster prior-authorization decision timelines take effect and metric collection begins; by March 31, 2026, the first public prior-auth performance metrics are due; and by January 1, 2027, the required FHIR APIs must be live in production with managed-care programs aligning to their rating periods.
Stay in touch
Subscribe to get insights from FHIR experts, new case studies, articles and announcements
Great!
Our team we’ll be glad to share our expertise with you via email





