
If you’ve worked in healthcare long enough, chances are you’ve run into the frustration of prior authorization. Originally designed to ensure patients get safe and necessary treatment, it’s become one of the most significant sources of delays, paperwork, and friction between providers and payers. The process is supposed to help, but too often it slows things down, sometimes to a harmful degree.
Providers spend hours chasing approvals. Payers wade through incomplete documentation. And patients? They’re stuck waiting—sometimes days—for treatments or medications they need now. Everyone agrees the system isn’t working the way it should.
The good news: it doesn’t have to be this way. The path forward lies in two things: automation and standardization. Automating prior authorization removes unnecessary delays. Standardizing data exchange through HL7 FHIR (Fast Healthcare Interoperability Resources) makes that automation scalable, accurate, and easier to implement across systems.
In this article, we explore what that looks like in practice, why it matters for payers, providers, and patients, and how Edenlab helps make it happen.
Highlights:
- Manual prior authorization costs the U.S. healthcare system an estimated $25 billion annually.
- 95% of physicians say the prior auth process contributes to burnout.
- Automation reduces prior authorization processing time by up to 90%.
- AI tools can handle 50–75% of manual prior authorization tasks.
- The CMS-0057-F Final Rule mandates FHIR-based APIs for prior auth by 2027.
Why Prior Authorization Still Matters
Let’s be real, the prior authorization process isn’t anyone’s favorite part of healthcare. For providers, it’s a time sink. For payers, it’s a logistical mess. For patients, it’s often the reason their treatment gets delayed. And yet, despite all the frustration, prior authorization still plays a vital role in keeping care aligned with what’s necessary, safe, and effective.
It’s meant to act as a checkpoint. Before approving expensive procedures or prescriptions, payers want to ensure solid medical reasoning behind the choice. In theory, it supports smarter, evidence-based care and helps reduce waste. It can promote better outcomes when aligned with value-based care models by encouraging providers to follow clinical guidelines.
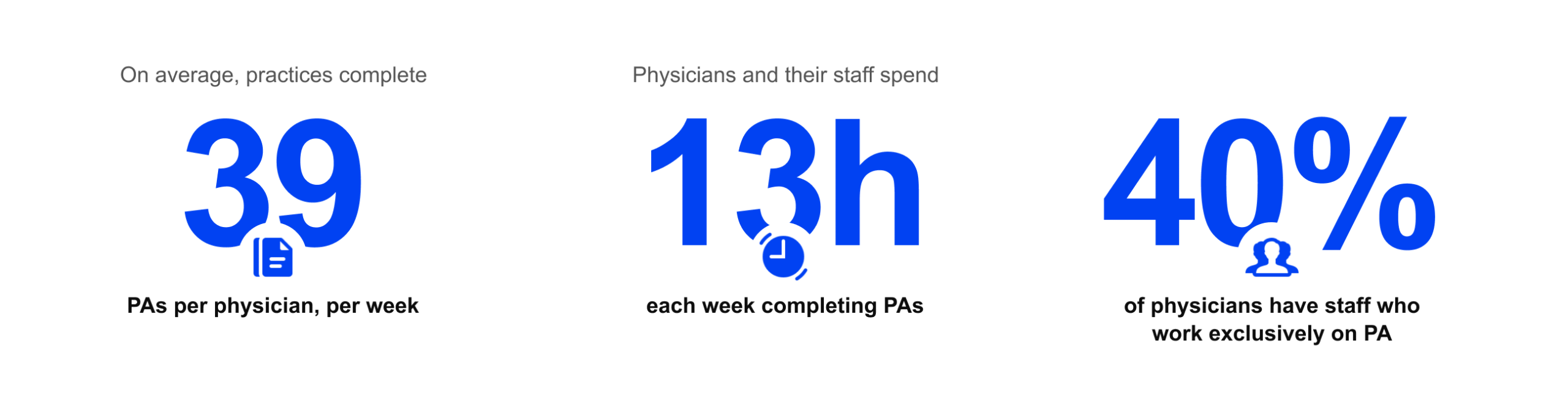
But here’s the problem: the way prior authorization is done today is stuck in the past. Too many workflows still revolve around faxes, disjointed web portals, and manual prior authorization form-filling. None of it fits into the modern clinical routine. As a result, providers and their teams spend around 14 hours each week just trying to get approvals. That’s time not spent with patients. And the financial cost? In the U.S. alone, the healthcare system spends about $25 billion annually on manual prior authorization workflows. Meanwhile, patients are left waiting—sometimes too long—for their needed care. And that’s a serious disconnect for something that’s supposed to protect them.
Beyond the financial burden, the human cost is even more troubling—nearly all physicians (95%) report that the prior authorization processes significantly contribute to burnout. A third of them say they have seen delays resulting in serious patient adverse events. And the downstream effects of inefficiency are substantial: 87% of physicians report that poor PA (prior authorization) workflows drive up overall utilization, with patients requiring repeat visits, additional procedures, or even emergency care due to delayed or denied approvals. Hospitals also bear the impact, with as much as 12% of their revenue at risk from denied claims, many of which are tied to prior authorization mismanagement.
These issues aren’t anomalies. They’re systemic indicators of a broken process. Without modernization, structured data, real-time exchange, and intelligent automation, prior authorization will continue to obstruct the objectives it was supposed to support.
Looking to streamline your revenue cycle management?
Check our
Claim & Billing solution development servicesWhat Automated Prior Authorization Actually Delivers
The difference is hard to ignore when you take prior authorization out of the slow lane and make it work the way it should.
For providers, automation means fewer headaches and more time with patients. Instead of chasing approvals across portals and paper forms, requests can be triggered directly from the EHR. According to the American Medical Association, this kind of integration can cut time spent on prior authorization tasks by up to 90%. That’s up to 13 hours a week saved for doctors and staff—time that can be reinvested in actual care. With fewer interruptions and clearer workflows, the administrative burden drops by up to 40%.
Payers benefit just as much. With structured, standardized information coming in through electronic systems, processing becomes three to five times faster. There’s less back-and-forth, fewer errors, and far fewer denials due to incomplete data, cut in half, by some estimates. Automated systems also help apply clinical rules more consistently, boosting approval accuracy.
That’s exactly what Edenlab delivered for Heals.Asia, one of the largest TPAs in Hong Kong, building a FHIR-based auto-adjudication engine that evaluates claims and pre-authorizations against complex plan rules like deductibles and co-pays. The result? Faster decisions, reduced manual effort, and a system that fits into existing business processes without disruption.
Patients, of course, feel the downstream effects. They’re not left in limbo waiting for treatment approvals. In fact, prior auth automation can shorten wait times for diagnostic tests and therapies by as much as 50%. It also means fewer calls to providers’ offices—down by 60% in some systems—and a greater likelihood of sticking with prescribed care plans. Faster approvals mean faster care, and that leads to better health outcomes.
When done right, prior authorization doesn’t have to be a hurdle. It can silently promote better, safer, and more coordinated care while remaining out of the way.
How Prior Authorization Works for Services vs. Meds
Prior authorization on FHIR plays out in two very different ways, depending on whether you approve a service or a medication.
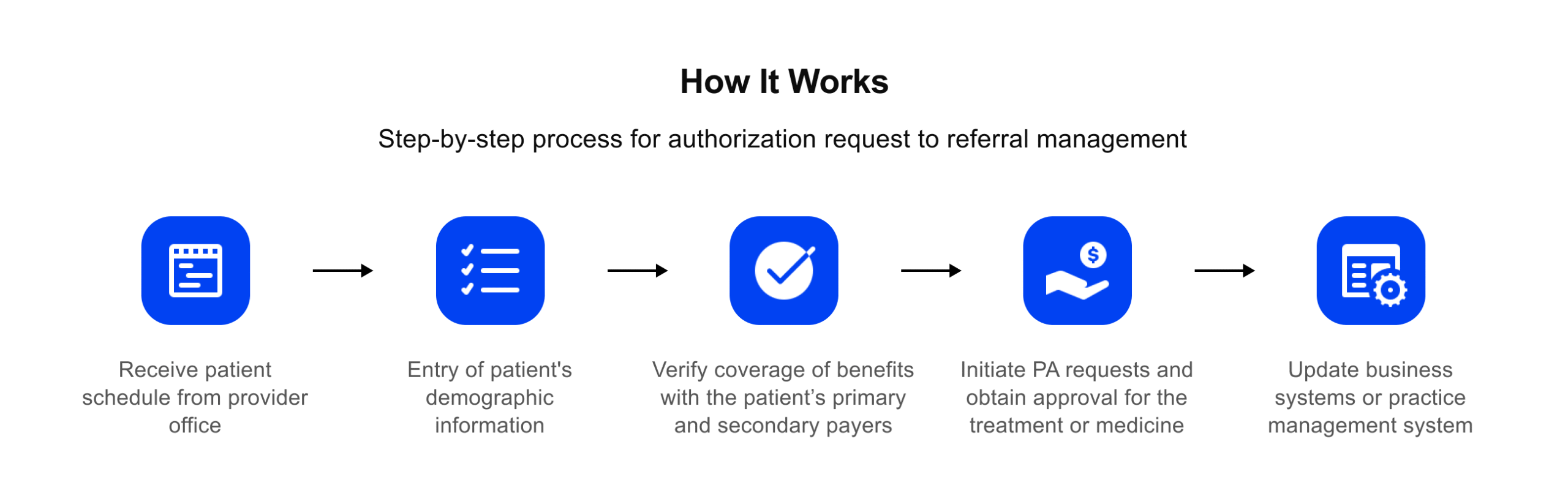
Let’s say a provider orders a service like an MRI or refers a patient to a specialist. The prior authorization process usually kicks off right there in the EHR. The system should flag that authorization is needed, pull in relevant clinical notes, and package everything into a request that meets the payer’s requirements. If it’s working well, the provider barely notices—it just fits into the flow of the visit.
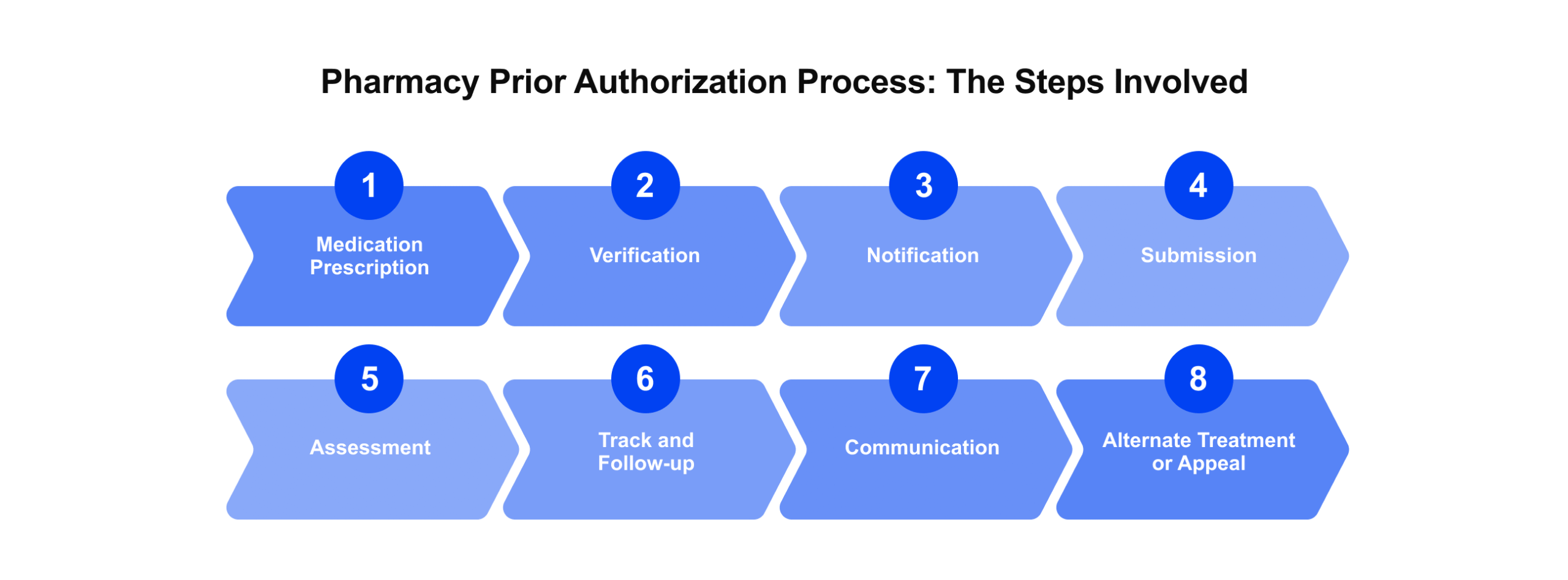
Now compare that to prescriptions. These authorizations often happen at the pharmacy or during e-prescribing, where timing is everything. If the system can’t confirm coverage fast or suggest a covered alternative, the patient may walk away without their meds. That missed pickup? It’s not just an inconvenience—it could impact their recovery.
These are two different worlds with the same underlying challenge: making sure care gets to the patient without unnecessary delays. That’s why flexible automation is so important, grounded in a shared standard like FHIR. It allows both types of workflows to run smoothly, without forcing everyone into the same mold.
Need expert assistance with ePrescribing?
We’re here to help. Explore how we can assist you in designing secure, compliant, and scalable solutions. Check our
E-prescribing solutions development servicesWhy FHIR Changes the Game
Prior authorization can’t be fixed with better paperwork. What’s needed is a common language, and that’s what the FHIR standard brings to the table.
FHIR provides a modern framework for systems to exchange healthcare data in real time. It replaces patchwork integrations and fragmented data sharing with structured, standardized, and API-driven exchange that works across platforms. This enables payers and providers to communicate using the same format, reducing confusion and manual rework.
More importantly, FHIR supports the specific workflows that make automated prior authorization possible. Da Vinci Project use cases like Coverage Requirements Discovery (CRD), Documentation Templates and Rules (DTR), and Prior Authorization Support (PAS) are all built on FHIR. Together, they allow systems to detect when prior authorization is needed, pull in the right clinical data, and send a request in a format the payer understands—automatically and in real time.
At Edenlab, we’ve built deep expertise around FHIR through national-scale projects and complex implementations. We know how to make these tools technically compliant and operationally effective. Whether you’re a provider looking to embed prior authorization into clinical workflows, a payer or TPA seeking to automate approvals across networks, or a product team building a new solution from day one, our FHIR development services are built to meet your real-world needs and ensure long-term compliance.
FHIR isn’t just a standard—it’s the key to making prior authorization finally work the way it should: fast, predictable, and invisible to the patient.
Regulations Are Driving the Shift
FHIR prior authorization has long been a sticking point in healthcare, costing time, money, and patient trust. Today, change is being driven not only by better technology but by regulation. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) sets a clear path forward: US-based payers must embrace FHIR-based APIs that make prior authorization faster, clearer, and more connected.
Prior authorization requests must be addressed within seven days or 72 hours for essential cases by payers such as Medicare Advantage plans, Medicaid, and ACA issuers beginning in 2026. They must offer secure APIs that enable real-time access to claims, encounters, and prior authorization data by 2027. The purpose of these requirements is to provide patients and providers with a more comprehensive understanding of the situation, eradicate redundant documentation, and reduce delays.
Notably, the rule aligns with HL7 Da Vinci Project implementation guides. The Da Vinci Project is an industry-led initiative that defines how to implement automated prior auth workflows using FHIR. Its three key implementation guides—CRD (Coverage Requirements Discovery), DTR (Documentation Templates and Rules), and PAS (Prior Authorization Support)—work together to let providers check if prior auth is needed, gather required documentation automatically, and submit a prior authorization request electronically, within their clinical systems.
Why does this matter so much? Da Vinci prior authorization is a process that connects multiple players: payers, providers, TPAs, and sometimes pharmacies. Without shared standards like FHIR, these connections break down. That’s why CMS is pushing for interoperability for coordinated, value-based care.
These guides are powered by specific FHIR resources, which enable automation and standardization. CRD relies on resources like CoverageEligibilityRequest, DeviceRequest, and ServiceRequest to trigger checks for prior auth requirements. DTR uses Questionnaire, Observation, and DocumentReference to collect the clinical data needed for submission. PAS enables actual submission through Claim and receives responses via ClaimResponse, while supporting X12 278 conversion where necessary.
Edenlab’s experience in regulation-driven, FHIR-based development makes us a trusted partner in this transition. Our Kodjin platform is ONC- and gematik-certified, proving its readiness for national-scale, compliant deployments. With Kodjin, we’ve built robust FHIR-native systems that meet CMS and ONC compliance mandates, support Da Vinci implementation, and enable seamless automation across claim adjudication, e-prescribing, and prior authorization workflows. From mapping legacy data to FHIR resources like CoverageEligibilityRequest and Claim to building real-time provider APIs, Edenlab helps payers and providers meet regulatory deadlines while building future-ready infrastructure.
What FHIR Prior Authorizations Solutions Exist Today
Prior authorization automation comes in four main flavors:
- Embedded in EHR systems. Many modern EHRs now include prior auth modules that let clinicians place an order, check eligibility, and submit requests—all without leaving the patient chart. Some even support Da Vinci workflows like CRD, DTR, and PAS to keep compliance in place and clicks to a minimum.
- Integrated within ePrescribing platforms. Systems like Surescripts, Veradigm, and DrFirst perform real-time formulary checks, alert prescribers when prior authorization is required, and suggest covered alternatives.
For instance, Edenlab built Ukraine’s national e-Prescribing system from the ground up, turning what used to be a paper-heavy, delay-prone process into a fast, digital-first service. Today, over 15,000 pharmacies use the system, with more than 75 million e-prescriptions issued and 1.6 million added each month. Doctors can create prescriptions electronically, patients receive medications using a simple code, and pharmacies report transactions instantly. For the government, this means real-time visibility into medication usage, streamlined reimbursements, and a major drop in fraud risk. - Part of RCM and claim adjudication tools. These platforms automate the full billing cycle, connecting eligibility checks, prior authorization, claims submission, and payment. Many support both FHIR APIs and legacy X12 formats to match various payer ecosystems.
- Dedicated ePA (electronic prior authorization) solutions. These standalone tools are designed solely for automating prior authorization. They’re ideal when your EHR or billing system doesn’t support PA or when you need flexible rules across multiple payers.
But no matter the product, one constant remains: off-the-shelf tools rarely match your real-world needs. Each payer, provider, or TPA has unique policy frameworks, approval pathways, and documentation workflows.
That’s where Edenlab adds real value. We work with product developers to create FHIR-native, regulation-ready prior authorization modules, whether launching new solutions or upgrading existing ones, especially for national-scale digital health systems like HIEs. And for providers or payers bringing in third-party PA tools, we customize and integrate them to fit your internal processes, ensuring that adoption is seamless, compliant, and built for scale.
What’s Next: AI, Clarity, and a Process That Finally Works
Prior authorization using FHIR has long been a dreaded step in care delivery, but that’s finally changing thanks to AI and better data standards.
McKinsey estimates that AI can handle 50–75% of the manual tasks involved in prior authorization, freeing clinicians to focus on complex cases and direct patient care. Instead of wading through dense policy PDFs, AI systems can now read, interpret, and extract payer rules, helping providers know exactly what’s required up front and reducing needless denials.
We’re also seeing tools that auto-collect relevant clinical data, intelligently structure it, and attach it to requests—so providers don’t have to sift through charts. It’s about delivering a clean, complete submission on day one, not after three follow-ups.
On top of that, there’s a push toward explainable AI systems that don’t just say yes or no, but also show their reasoning. That matters when care decisions are on the line: transparency builds trust, cuts appeals, and creates opportunities to learn and improve.
But none of this magic would work without structured, FHIR-based data. Without it, AI is left guessing. With it? We can build smart, context-aware workflows that learn and adapt over time, improving with every use.
Through Edenlab’s FHIR-first infrastructure, we’re helping clients integrate AI-ready pipelines, embed decision support into e-prescribing and claims systems, and deliver clinical workflow automation services that reduce friction, boost clarity, and improve care.
Conclusion
Prior authorization doesn’t have to be a bottleneck. With the right mix of automation, FHIR-based standardization, and regulatory alignment, it can become what it was meant to be—a safeguard for appropriate care, not an obstacle.
The good news is that the path forward is clear. We have the tools to fix it, and the industry is finally moving in that direction. Automation reduces manual workload. FHIR makes data exchange standardized, reliable, and scalable. Regulatory pressure, from rules like CMS-0057-F, is creating real momentum. And AI prior authorization in healthcare is adding speed, structure, and transparency to what used to be a black box.
But these changes won’t implement themselves. Whether you’re a provider trying to embed prior auth into everyday clinical workflows, a payer or TPA managing thousands of requests, or a product team building a new digital health tool, success depends on getting the technology, the standards, and the strategy right.
That’s where Edenlab comes in. We’ve helped national health systems, payer platforms, and product teams modernize prior authorization using FHIR-first, regulation-ready architecture. From real-time eligibility checks and pre-auth automation to AI-ready infrastructure and complete CMS/ONC alignment, we know what it takes to make these systems not only work, but work at scale.
Prior authorization can be faster. It can be smarter. And it can be invisible to the people it’s supposed to serve: patients.

Ready to make prior authorization work for your organization?
At Edenlab, we don’t just automate processes—we build scalable, compliant, and future-ready solutions tailored to the realities of payers, providers, and product teams. Whether you're modernizing an existing system or building from scratch, our team brings the healthcare-specific expertise needed to do it right.
FAQ
How long does it take to implement a FHIR-based prior authorization workflow?
It really depends on your starting point. If you’re building a complete workflow—eligibility checks, document gathering, and submission—you’re typically looking at a 3–6 month timeline from kickoff to go-live. If you start with just one piece, it could be up and running in as little as 6–12 weeks.
Do I need to replace my existing EHR to adopt FHIR-based prior auth?
Not at all. You can layer FHIR-powered automation on top of your current system. Most EHRs today support it or can be adapted. That means eligibility checks, clinical data gathering, and submission can all happen alongside your current workflow—no need for a rip-and-replace.
What compliance standards does Edenlab follow for payer–provider integrations?
We build to industry standards—SMART-on-FHIR, US Core, and the CMS prior authorization API spec, aligned with Da Vinci CRD/DTR/PAS guides. Our platform is ONC-certified and designed to meet payer–provider integration requirements out of the box.
Can Edenlab help with testing and certification for FHIR workflows?
Yes, we support full-level testing, using tools like Inferno and commercial test suites to ensure conformance. We help prepare documentation, manage AppRegistry registration, and work alongside labs to help you complete certification.
What if we only want to automate part of the prior auth process?
That’s fine, automation can be modular. You can start with eligibility checks or documentation tools and expand later. Kodjin’s architecture lets you add components as needed without rebuilding from scratch.
Stay in touch
Subscribe to get insights from FHIR experts, new case studies, articles and announcements
Great!
Our team we’ll be glad to share our expertise with you via email







