
Effective data mapping in healthcare is a cornerstone of interoperability, yielding best-in-class security and compliance, high clinician trust, and global adoption in clinical settings. These outcomes underscore the essential role of robust data mapping for patient care and healthcare operations. However, achieving seamless data exchange remains challenging.
This is exactly where AI data mapping in healthcare is increasingly positioned as a practical enabler, not just a buzzword.
The global healthcare ecosystem is shifting toward interoperability-first strategies, yet converting proprietary data formats and local codes into standard terminologies and data models (like SNOMED CT, LOINC, ICD-10, RxNorm) is a major bottleneck.
Mapping local codes to standard terminologies requires specific expertise and is time-consuming, often requiring additional investment without clear immediate ROI. As a result, healthcare organizations still struggle with siloed data and high integration costs — even a few years ago, only 62% of U.S. hospitals could effectively share patient data, leaving nearly 40% mired in incompatible systems.
Data mapping is the unsung hero enabling true interoperability, but historically it’s been a manual, tedious, and resource-intensive process.
Amid these challenges, artificial intelligence (AI) is emerging as a game-changer for data mapping. AI-powered mapping introduces a faster, scalable, and more consistent approach that can transform how healthcare software providers and data teams operate, including AI-based healthcare data mapping initiatives that reduce reliance on hand-built rule sets.
This article explores the limitations of traditional data mapping and how AI is addressing them, ultimately revolutionizing healthcare interoperability.
Highlights
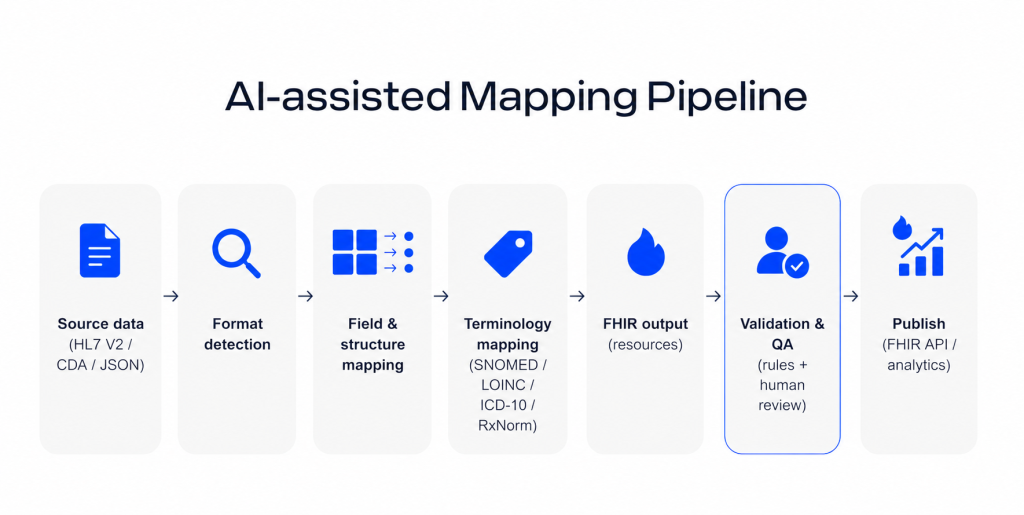
- AI can accelerate HL7-to-FHIR and standard terminology mapping by reducing repetitive manual work and shortening integration timelines.
- Traditional healthcare mapping is slow, brittle, and expensive to maintain across legacy systems, local codes, and changing standards.
- The real value of AI mapping is not full automation, but faster first-pass transformations with better consistency and human validation.
- Organizations that combine AI-assisted mapping with governance and expert oversight can scale interoperability more efficiently and with less operational overhead.
The Problem with Traditional Data Mapping
In today’s healthcare IT environment, data originates from diverse sources — legacy EHRs, lab systems, devices — often in incompatible formats (e.g. HL7 v2 messages, proprietary CSVs, custom JSON). Traditionally, making these talk to modern standards (like FHIR®) involves painstaking manual mapping of each data element.
Skilled domain experts must define how each field in the source format translates to the target format, often by writing or configuring hundreds of mapping rules for every message type.
This process is time-consuming, costly, and error-prone. It can take months to build and test a single mapping template for something like an HL7 v2 ADT message to a FHIR Patient Resource. Each new format or use case demands a fresh set of rules. This high dependence on specialized FHIR engineers or integration analysts creates a bottleneck.
Human experts can introduce inconsistencies, and variations in how different hospitals implement standards (or use local codes) make one-size-fits-all solutions impossible. As a result, traditional mapping projects often run over schedule and over budget, struggling to keep up with growing interoperability needs.
Conventional data mapping workflows also require the source standard and format to be explicitly known and handled in advance. Mapping tools or engines cannot generally autodetect an unknown format — an extra layer of logic must identify the incoming data type (HL7 v2 vs. CDA vs. custom JSON, etc.) and route it to the correct mapping rules.
This adds complexity and points of failure. Moreover, custom-coded mappings demand ongoing maintenance: whenever a source system changes or standards update, experts have to manually adjust the mapping scripts.
These factors slow down projects and reduce agility. Many healthcare providers have amassed fragmented mapping solutions — a patchwork of interface engines, custom scripts, and hard-coded tables — which are difficult to manage and scale.
In practice, this has led to rising integration costs (up to 30% of IT budgets in some cases) and a cycle of costly dependency on interface vendors or consultants. Even then, interoperability isn’t guaranteed; nearly 40% of hospitals still grapple with incomplete data exchange. This is why many organizations are now evaluating using AI for data mapping in healthcare as an operational necessity rather than an experiment.
In short, the traditional approach to data mapping struggles to meet modern demands for speed, scalability, and real-time data sharing.
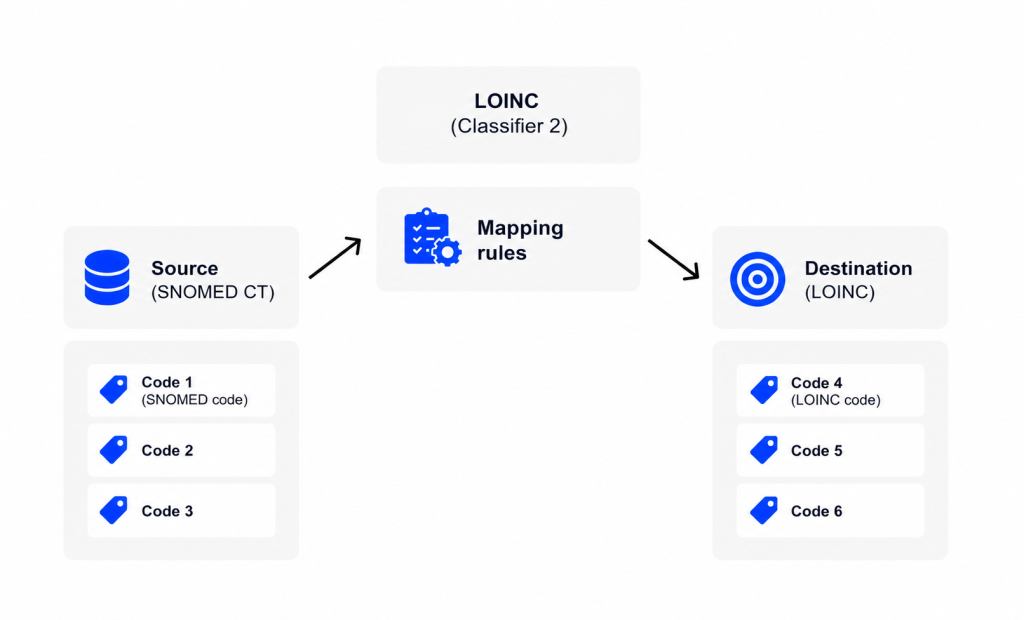
Example: HL7 v2 to FHIR Mapping Challenges: Consider the task of converting an HL7 v2 message (a legacy text-based standard) into a FHIR resource (a modern JSON/XML standard). A traditional mapper would require a pre-built mapping template for each message type (e.g. ADT^A01 — patient admission). The template might contain thousands of rules mapping HL7 segments and fields to FHIR elements, plus logic to translate codes (e.g. local lab codes to LOINC).
Such mapping rules are typically written by hand, thoroughly tested, and versioned. If an incoming message deviates slightly (say a custom segment or an unexpected value), the mapping might fail or produce incorrect output. Handling these edge cases means more manual rules. Clearly, this process is brittle and hard to scale. In contrast, AI-based data mapping in healthcare aims to generalize across these variations by learning patterns from real-world examples rather than hard-coding every exception.
Struggling with fragmented interfaces and mapping maintenance?
Build an integration layer designed for change: standards-first, observable, and secure.
Healthcare integration solution developmentHow AI Changes the Mapping Game
AI is transforming data mapping from a static, rule-based exercise into a dynamic, model-driven process. Instead of relying on humans to predefine every mapping rule, AI systems (particularly those leveraging machine learning and natural language processing) can learn from data and make intelligent mapping decisions.
In practice, AI for data mapping in healthcare is less about “replacing integration teams” and more about reducing repetitive work while improving consistency. Here’s how AI disrupts the status quo:
Automatic Format Recognition
Advanced AI models can analyze incoming data and infer its format and structure. For example, a trained model might distinguish an HL7 v2 message from a CDA document or a custom JSON simply by parsing its syntax and content patterns.
This means an AI-enabled mapper could auto-detect the source format, reducing the need for a separate preprocessing layer to tell the system what kind of data it’s dealing with. The AI effectively brings built-in knowledge of healthcare data standards. This capability is a core driver behind broader adoption of healthcare data mapping using AI in integration-heavy environments.
Handling Unstructured Data
Traditional mapping largely focused on structured fields, but healthcare also contains unstructured text (clinical notes, scanned documents). AI excels at bridging this gap. Techniques like natural language processing (NLP) enable extracting key information from free text and incorporating it into structured formats.
For example, AI can read a scanned clinical note or a PDF and convert relevant pieces into FHIR resources. This extends data mapping beyond just structured interfaces, allowing previously untapped data (like physician notes or faxed reports) to be mapped into standard data models.
The result is a more complete and rich dataset flowing through your systems than what manual mapping alone could achieve, including more realistic support for clinical data mapping with AI across mixed structured/unstructured sources.
Speed and Efficiency
Automation of repetitive mapping tasks means data conversions happen faster. AI dramatically reduces manual effort and accelerates the conversion process, making standard adoption (like FHIR) faster and more cost-effective.
Scalability
AI mapping solutions learn from each new example, improving over time. They can be scaled to handle growing data volumes or new formats without a linear increase in human labor. Organizations can onboard new data sources or exchange partners quickly, since the AI model can adapt to mappings it hasn’t seen before. This scalability is crucial as healthcare data keeps exploding in volume and diversity.
Consistency and Accuracy
By leveraging training on large datasets and patterns, AI can apply consistent logic to mappings, reducing the variability that comes with different human coding rules. It can also catch complex relationships that rule-based approaches might miss.
AI semantic mapping can automatically resolve structural differences and even standardize terminologies, minimizing the risk of human error. Fewer manual touchpoints translate to fewer mistakes and mismatches. In fact, automating the process with AI leads to fewer human errors and improved data quality.
Cost Savings
With less need for custom development and maintenance, AI-driven mapping promises cost efficiencies. It lowers the dependency on specialized interface engineers for every new project. The interoperability gains can be achieved with smaller teams, and organizations can reallocate budget from labor-intensive mapping efforts to other strategic initiatives. Over time, adaptive AI mappings also mean less rework as standards evolve, further containing costs.
Consolidated Workflows
AI mapping can consolidate multiple steps (parsing, transforming, code translation, validation) into one intelligent pipeline. For example, AI can automate message parsing, suggest optimal FHIR mappings, and even validate the converted data in one go.
This reduces reliance on a patchwork of tools. Instead of using one tool to identify format, another for field mapping, and yet another for terminology translation, an AI-enabled platform can handle many of these within a unified system. Fewer moving parts simplify maintenance and monitoring, and they also create a clearer path to AI-based FHIR data mapping within a governed integration pipeline.
Impact on Teams
The introduction of AI in data mapping profoundly changes team dynamics. Domain experts and integration specialists are no longer spending their days writing mapping tables or troubleshooting countless interface rules. Instead, their role shifts to providing guidance and oversight. In AI mapping projects, domain experts help train the models (by feeding example mappings, fine-tuning responses, and validating outputs).
They become supervisors who review AI-generated mappings for accuracy rather than manual mappers of every field. This frees up valuable human expertise to focus on high-value work — refining workflows, handling complex edge cases, and improving data governance — instead of doing rote translation tasks.
AI doesn’t remove humans from mapping. It removes repetitive rule-writing and shifts experts to validation, governance, and edge-case handling.
Meanwhile, IT teams and data engineers benefit from faster project cycles and can deliver integrations in weeks instead of months. They can also involve less-technical staff in mapping efforts via AI-assisted interfaces (e.g. a tool that lets a user upload a sample file and get a first-pass mapping suggestion from the AI).
Overall, AI makes the mapping workflow more accessible and less siloed. Technical product owners and CTOs see faster interoperability outcomes, and analytics teams get timely access to unified data without waiting forever for pipeline development. In short, AI doesn’t remove humans from the loop, but it elevates their role and boosts productivity across the board.
Can AI Replace Traditional FHIR Mappers?
The advent of AI in data mapping naturally raises the question: will AI fully replace the need for human FHIR mappers and integration engineers? The short answer: is not entirely, at least not yet. AI drastically reduces the manual workload and can handle many mapping tasks autonomously, but human expertise remains vital for certain aspects:
Need for Validation and Quality Assurance: Healthcare data is high-stakes. Errors in mapping (such as misinterpreting a lab result unit or mapping a code incorrectly) can have patient safety implications or regulatory repercussions. AI models, while powerful, are not infallible. They may occasionally produce incorrect mappings, especially for edge cases or ambiguous data.
Therefore, expert oversight is required to validate AI outputs. In current implementations, a human typically reviews the mappings the AI proposes.
For example, an AI system might generate several mapping proposals for a given input, and a user (with domain knowledge) chooses the one that best fits and then manually fine-tunes any complex parts that the model couldn’t handle.
This human-in-the-loop approach is crucial for maintaining accuracy and trust, especially when deploying AI FHIR data mapping at scale across multiple sites and partners.
Handling Complex and Novel Scenarios: There will always be unusual scenarios — a niche proprietary format, a highly custom data field, or a new standard release — where the AI model might not have sufficient training context.
Domain experts are needed to recognize when the AI is out of its depth and to provide the correct mapping logic or additional training examples. Traditional mappers bring deep contextual understanding (clinical, regulatory, local conventions) that complements AI’s pattern recognition.
Model Training and Tuning: AI models do not know every healthcare context out of the box; they require training data and ongoing tuning. Domain specialists and data engineers are needed to feed the model high-quality examples and correct it when it makes errors. In one case, AI specialists had to fine-tune a ChatGPT-based model by iteratively pointing out good vs. bad answers and providing additional context, which improved the model’s consistency.
This illustrates that building a robust AI mapper is an iterative collaboration between humans and AI. The knowledge of experienced mappers is embedded into the AI through this training process. As models mature, the nature of the expert’s job shifts from manually mapping data to teaching and supervising the AI.
In reality, AI-powered mapping complements traditional methods and roles. It takes over the repetitive, high-volume tasks that would otherwise bog down human integrators, enabling organizations to scale up interoperability efforts rapidly. At the same time, it elevates human roles to focus on strategy, oversight, and handling the exceptional cases.
Going forward, as AI models become more advanced and richly trained (potentially on vast amounts of healthcare data), we can expect the balance to keep shifting. The role of a “FHIR mapper” might evolve into that of an AI mapping supervisor or trainer. Experts will define governance rules, ensure quality, and update the AI’s knowledge as standards evolve, rather than hand-coding every transformation.
Conclusion
AI is undeniably transforming how healthcare data mapping is done. It brings speed, adaptability, and intelligence to a domain that was historically slow and manual. Early implementations show that AI can automate the bulk of HL7-to-FHIR conversions and similar tasks, accelerating project timelines and reducing costs.
Healthcare organizations adopting AI-driven mapping gain a competitive edge in achieving interoperability — they can integrate systems in days or weeks instead of months, respond faster to new data sharing demands, and ensure more consistent data quality across the board.
This has far-reaching implications: clinicians get more complete and up-to-date information at the point of care, IT departments can focus on innovation rather than low-level integration maintenance, and patients benefit from smoother information flow between the disparate systems that manage their health.
However, success with AI mapping requires recognizing its proper role. It is a powerful tool meant to augment human expertise, not replace it. The most effective solutions pair AI’s scalability with the guidance of healthcare data experts. Together, they overcome the old barriers of format fragmentation and coding mismatches.

Need faster, safer mappings to FHIR and standard terminologies?
Tell us your source formats and target use cases, and we’ll propose an implementation approach and validation workflow.
FAQs
Is AI mapping compliant with healthcare data regulations?
It can be, but compliance depends on how you deploy and govern it: access controls (RBAC/ABAC), consent, audit logs, encryption, data residency, vendor/BAA/DPA terms, and a human-in-the-loop QA process. AI itself isn’t “automatically compliant” without those controls.
How accurate is model-driven mapping compared to manual?
For common, well-represented patterns it can reach manual-level accuracy and often be more consistent; for edge cases (local codes, unusual HL7 variants, ambiguous fields) it needs review and validation. The right comparison is measured: precision/recall on a labeled test set and clinical/terminology QA.
Can I integrate Kodjin into my existing EHR pipeline?
Yes. Kodjin can typically be placed as the FHIR layer alongside your existing interfaces: ingest via your current engine/ETL, transform to FHIR, then expose/consume through FHIR APIs (and optionally events/queues). Most teams do this incrementally (FHIR facade/gateway pattern) rather than replacing the whole pipeline at once.
Stay in touch
Subscribe to get insights from FHIR experts, new case studies, articles and announcements
Great!
Our team we’ll be glad to share our expertise with you via email







