
The Observational Medical Outcomes Partnership (OMOP) has emerged as a common foundation for portable healthcare analytics. Today, OMOP in healthcare is becoming the standard approach for organizations that need interoperable, research-ready data across institutions.
Healthcare has been digitized, but healthcare analytics has not become portable. Every hospital network, every registry, every research consortium in Europe builds its insights on top of a specific database schema. Move to a new source, a partner site, a new study, a federated query from across the border, and most of that analytical work has to be rebuilt from the ground up. The answer the field has converged on is OMOP.
Who is this article for? European organizations engaged in observational research — pharmaceutical RWE teams, research divisions in hospitals and academic medical centres, data stewards working on EHDS readiness, and Health IT vendors whose customers are asking for OMOP-compatible outputs. If your work touches “how do I move data into and out of OMOP reliably, at production scale,” this is for you.
Highlights:
- OMOP makes healthcare analytics shareable, repeatable, and research-ready.
- EHDS is pushing European teams to treat OMOP readiness as infrastructure work.
- FHIR® moves clinical data; OMOP makes it usable for analytics and evidence generation.
- Edenlab helps teams move data into, out of, and around OMOP with Kodjin Data Platform.
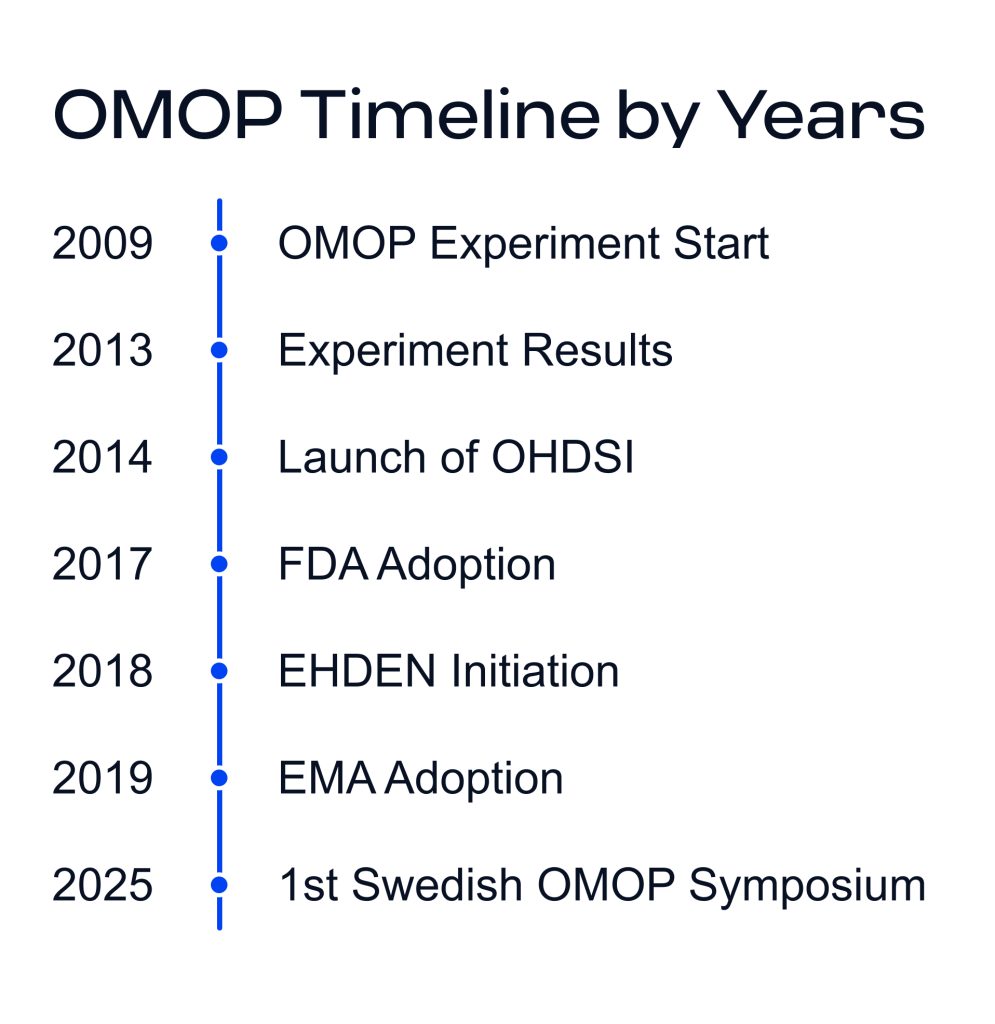
OMOP began in 2008 as a US public-private initiative focused on drug safety surveillance, and the problem it set out to solve was exactly this: “How do you analyze observational health data across institutions whose source systems have nothing in common?”.
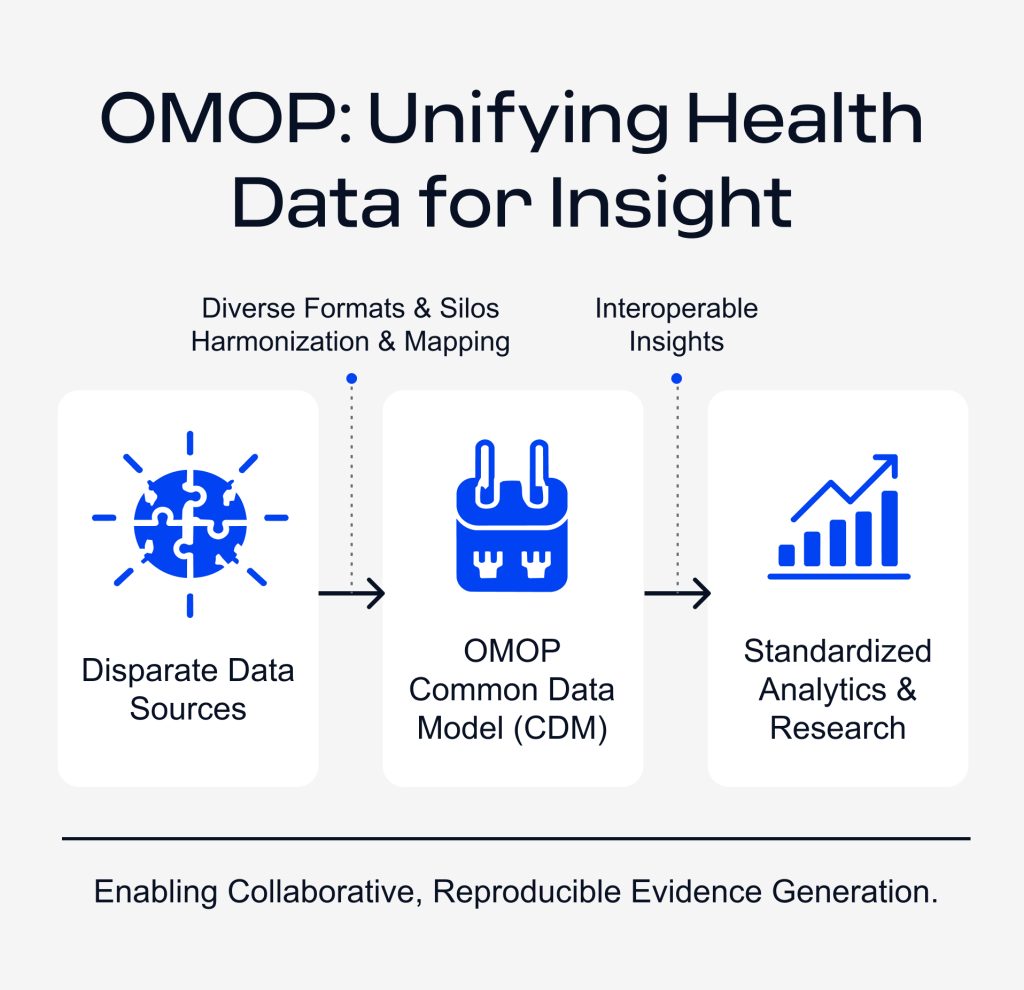
The answer was a shared model — a single canonical structure and vocabulary that any organization can convert its data into. The OMOP data model is designed for observational health data — the messy, real-world data from electronic health records (EHRs), claims systems, registries, and biobanks. By forcing this data through a common structure, analytical code can be written once and executed across many independent databases.
By the end of 2024, 544 standardized data sources across 54 countries had been converted to the OMOP CDM, covering approximately 974 million patient records — roughly 12% of the world’s population. The European Health Data Space (EHDS) Regulation entered into force on 26 March 2025, with most secondary-use provisions becoming applicable from March 2029.
Why engage with EHDS at all? Beyond regulatory obligation, EHDS opens concrete benefits: participation in pan-European research networks like DARWIN EU and EHDEN, standardized permitting processes across member states, a recognized path for secondary use of clinical data, and EU-funded infrastructure that lowers the cost of becoming research-ready. Organizations that prepare early sit inside the network rather than scrambling to catch up.
Where Edenlab fits. Edenlab has been doing this work in production for years. Our FHIR-to-OMOP pipeline for the Ludwig Boltzmann Institute is one example of the architecture this article describes. We combine IT consulting expertise with our own products — Kodjin FHIR Server and Kodjin Analytics — to move clinical data into, out of, and around OMOP for European research and EHDS contexts. For broader support, see our healthcare data analytics services.
Why Healthcare Research Has Been Stuck in Silos
The default architecture for hospital analytics looks the same almost everywhere. A clinical data warehouse sits behind a custom schema, and a team of analysts builds queries, dashboards, and cohort logic against it. Years of institutional knowledge accumulate inside those queries.
Then something changes. A new study requires data from three partner hospitals. A pharma sponsor wants real-world evidence across four countries. The existing analytics doesn’t travel because the schemas at the other sites don’t match. This is a familiar problem across big data analytics in the healthcare industry: the value of data depends on whether teams can interpret, compare, and reuse it across systems.
Three structural problems compound this:
- Heterogeneous data elements and source vocabularies. The same concept, blood glucose, a hypertension diagnosis, or a metformin prescription, is recorded differently in every system, with different code sets, granularity, and quality.
- No shared analytical structure. Cohort definitions, study protocols, and statistical scripts assume a specific database layout. Move the layout, and the analytics have to be rewritten.
- Governance friction. Even when sites are technically willing to collaborate, the absence of shared standards turns every research partnership into a months-long alignment exercise on terminology and data governance.
Standardizing the underlying model removes the friction. If every participating site holds its data in the same shape, the same cohort definition can run anywhere without rewriting. That is the conceptual shift behind standardized data in healthcare, and it is what makes federated research networks technically possible.
What Is the OMOP Method?
The OMOP CDM defines a fixed relational structure — person, visit, condition occurrence, drug exposure, measurement, observation, and so on — and pairs it with a standardized vocabulary layer that maps source codes (ICD-10, SNOMED CT, LOINC, RxNorm, local dictionaries) into a shared conceptual space.
The analytical value of standardized OMOP data
Once data is in OMOP CDM, research teams gain a shared analytical foundation that makes collaboration more consistent:
- The same study protocol runs across multiple sites, and the results compare like-for-like.
- The OHDSI open-source ecosystem — Atlas for cohort design, HADES for population-level estimation, PatientLevelPrediction for ML pipelines — works out of the box.
- Reproducibility and quality evaluation become structural properties of the analysis rather than something each team has to engineer.
- Cross-institutional research and federated sharing of insights become operationally feasible.
This is what OMOP healthcare analytics looks like at scale — a shared, comparable, reproducible substrate for evidence generation. That shared structure also creates better conditions for advanced analytics in healthcare, where cohort logic, prediction models, and outcome evaluation need consistent data definitions across sites.
How EHDS makes OMOP readiness a practical requirement
For years, adopting CDM healthcare standards was a strategic choice — a bet on the future of observational research, or a requirement of a specific consortium. The EHDS has reframed it.
Secondary use of health data is now a regulated activity across the European Union, with national health data access bodies, defined data permits, and expectations about the formats in which data is delivered to researchers.
The point of a cross-border health data network is that analytics can be executed across many nodes in the same way. That is not achievable if every node defines diabetes differently or codes medications in a local vocabulary. OMOP is the technical answer to the EHDS requirement. EHDS is the political driver; OMOP is the engineering substrate that lets the policy actually work.
Governance becomes part of the data model
Adoption of a shared analytical model changes how an organization handles consent, access control, audit, and privacy — the substance of healthcare integrated governance. Integrated governance in this context means treating data stewardship, regulatory compliance, and analytical access as a single coordinated discipline rather than separate teams handling separate questions.
The principles remain the same to research on patient data: lawful basis, minimized access, traceable use, and ethical review where required. The difference under EHDS is operational. These principles now have to be enforceable across nodes that share an analytical pipeline.
FHIR-to-OMOP: The Hidden Engineering Challenge
OMOP solves the analytical side of the problem; FHIR solves the operational side, moving structured clinical data between systems for care delivery and real-time apps. Most modern European Health IT investment has been pointed at FHIR.
The two standards cover different layers of the same stack — FHIR for operational exchange, OMOP for research and population health analytics.
A realistic European health data architecture needs both. And that creates a specific, often-underestimated engineering task: moving data between them. This is where healthcare interoperability services need to go beyond interface development and support the deeper semantic, vocabulary, and governance work behind reliable data exchange.
A FHIR-to-OMOP transformation involves vocabulary translation across multiple code systems, temporal alignment of clinical events, reconciliation of FHIR’s resource-graph model with OMOP’s normalized relational schema, and continuous handling of incremental updates.
It is a production engineering discipline, and Edenlab has built it at scale: the Ludwig Boltzmann Institute case study shows exactly this in operation — a FHIR-native data platform feeding an OMOP export pipeline that researchers consume directly.
The three use cases below describe the directions our customers most often need this work to flow.
Need expert assistance with interoperability?
We are here to help. Check our
Healthcare interoperability solution development servicesUse case 1: Discovery before you commit
The pain. You are planning a study. Before you sign contracts, allocate analyst time, and build out a full research pipeline, you need to know whether the data supports the question. Is the cohort viable? Are the exposures and outcomes recorded with enough fidelity? Is the question worth pursuing at this site?
In most environments, there is no fast way to answer this. Researchers wait weeks for a data extract, then spend more weeks discovering that the cohort is too small or the definitions don’t hold. The cost of finding out late is enormous.
The solution. Our own product, Kodjin Analytics, operates on top of your existing clinical data, ideally using FHIR, but is flexible across formats, letting researchers and data stewards explore the population, sketch preliminary cohorts, and validate that a study is feasible before any heavy engineering happens.
Because Edenlab’s platform can move data bidirectionally between FHIR and OMOP, the discovery phase and the formal research phase share the same underlying data without parallel pipelines or remapping work. For research-active hospitals and academic medical centers, this changes the economics of feasibility analysis from a multi-week procurement to a working session.
For organizations building their own analytical capabilities, this is also where medical analytics software development becomes more practical: teams can start with discovery, validate the data, and only then invest in full research workflows.

Use case 2: Packaging your data for EHDS
The pain. You hold operational data, often in FHIR, sometimes in a clinical data warehouse, occasionally in something more local, and you need to deliver it as OMOP. The driver might be EHDS compliance, a DARWIN EU participation request, a sponsored study, or a national health data access body.
Building a FHIR-to-OMOP pipeline in-house is months of engineering work, and that is before addressing vocabulary mapping, ongoing maintenance, and validation against OMOP quality checks. For most healthcare organizations, this is not core competence and not where internal engineering capacity should be spent.
The solution. The Kodjin Data Platform handles the FHIR-to-OMOP export end-to-end. Your operational data stays in FHIR; researchers and external data permits receive the OMOP-shaped extract; the transformation is maintained as a productized pipeline.
This is exactly what Edenlab did for the Ludwig Boltzmann Institute (LBI). LBI runs its clinical research data on a FHIR-native platform built by Edenlab; researchers access the data as OMOP.
The transformation is invisible to the research team and reliable enough to underpin a production research environment. For European hospital networks under EHDS deadline pressure, this is the shortest path between “we have FHIR data” and “we are an EHDS-ready node.”
Check out more of our healthcare analytics case studies.
Use case 3: Moving data out of OMOP
The pain. You already have OMOP data, perhaps from a legacy research collaboration, a national cohort, or a previous CDM project, and you need to use it somewhere else. A new study calls for FHIR-shaped input. An analytics product expects a different schema. OMOP is excellent as an analytical destination but less convenient when you need to leave it for an operational or product context.
The solution. Edenlab’s transformation engine is bidirectional. We process OMOP into FHIR, into Kodjin’s analytical model, or into bespoke target schemas. Once your data is in Kodjin, the full analytics stack, exploration, cohort definition, and federated query support become available regardless of whether the source was OMOP, FHIR, or something else.
In a real European data architecture, data doesn’t flow in one direction — a platform that moves it only one way forces every round trip to be rebuilt by hand.
The Same Engine, Three Directions
These three use cases are three directions of the same bidirectional engine:
- Into OMOP — when you need to prepare data for EHDS, DARWIN EU, sponsored studies, or any context where OMOP is the required delivery format.
- Out of OMOP — when you have OMOP data and need to move it into FHIR, into an analytics platform, or into a target system that does not speak CDM.
- Around OMOP — when discovery, analytics, and research live on the same underlying data, and the format depends on what you are doing at any given moment.
This is what shareable analytics actually requires in practice. A common data model healthcare standard is necessary but not sufficient — the engineering to move data in, out, and across formats at production scale is what turns OMOP’s theoretical interoperability into operational interoperability.
How Edenlab Helps Turn OMOP into Operational Infrastructure
Edenlab combines two things that the OMOP-and-EHDS transition tends to need together: deep IT consulting expertise in healthcare interoperability, and our own platform Kodjin, including the Kodjin FHIR Server and Kodjin Analytics, that handles the FHIR-to-OMOP work at production level rather than as a project artifact.
For RWE teams in pharma, research divisions in hospitals and universities, and data stewards working in the EHDS context, the practical question is “how do we get our data into and out of it without making this our internal engineering problem for the next eighteen months?” That is the question we are built to answer.
Talk to our team about your interoperability roadmap. Whether you are preparing for EHDS, scoping a research collaboration, or trying to make existing OMOP data useful in a new context, we can show you what a working bidirectional pipeline looks like and what it would take in your environment.

Prepare your data for the next stage of healthcare analytics
From FHIR-to-OMOP transformation to analytics-ready infrastructure, Edenlab helps clinical data teams make health data easier to share, study, and reuse across research networks.
FAQs
Can OMOP be implemented without replacing existing systems?
Yes. OMOP works as an analytical layer alongside your EHR, FHIR server, laboratory systems, and other operational tools. These systems continue to run as usual, while OMOP receives a structured analytical copy of the data through an ETL or streaming pipeline. For organizations already using FHIR, a FHIR-to-OMOP pipeline prepares data for research and secondary use without changing the operational layer.
What is the difference between OMOP and FHIR?
FHIR and OMOP serve different purposes. FHIR is an interoperability standard for exchanging clinical data between systems, supporting real-time use cases such as APIs, clinical applications, care coordination, and decision support. OMOP is a common data model for analytics that organizes clinical data into a standard relational structure, supporting cohort building, population-level analysis, observational studies, and Real-World Evidence research.
How can federated analytics improve research collaboration?
Federated analytics lets several organizations take part in the same study without moving raw patient data into a central database. Each site keeps data locally, usually in OMOP CDM, and runs the same study protocol against its own copy. Only aggregated results are shared back. This protects privacy, scales research across many institutions, and produces directly comparable results — the model used by DARWIN EU and EHDEN for cross-border research and secondary use of health data.
How does Edenlab help healthcare organizations become EHDS-ready?
Edenlab combines interoperability, data transformation, and analytics into one practical infrastructure. The work typically starts with a FHIR-native operational layer based on Kodjin FHIR Server, then layers in FHIR-to-OMOP (or proprietary-to-OMOP) transformation so organizations can deliver datasets in the format expected by EHDS bodies and research networks. Kodjin Analytics supports exploration and cohort discovery directly over FHIR or OMOP data.
Stay in touch
Subscribe to get insights from FHIR experts, new case studies, articles and announcements
Great!
Our team we’ll be glad to share our expertise with you via email







