
New health information exchange (HIE) initiatives often underestimate the complexity of integrating legacy repositories into an IDR backbone (in this guide, IDR stands for Integrated Data Repository) — a pitfall that has caused many projects to stumble or fail.
Healthcare data is notoriously siloed across disparate systems, and simply wiring them together is not enough to produce integrated data that can be safely reused across institutions. Challenges include mismatched data formats and semantics, lack of trust frameworks between competing organizations, network latency in retrieving distributed records, and the heavy lift of normalizing terminology across sources.
Building an HIE means addressing not just data transport, but also data quality, governance, and semantics, so you can integrate and store information in a governed repository system that supports APIs and analytics.
Integrating existing repositories is hard, and without careful planning for interoperability, many HIE projects have learned the hard way that “plugging in” legacy systems involves far more than technical interface work.
“Exchange” Beyond Basic Data Transport
In modern HIE contexts, “exchange” means more than just moving data from point A to point B. Early HIE efforts that acted as simple data pipelines or clearinghouses quickly found they provided insufficient value.
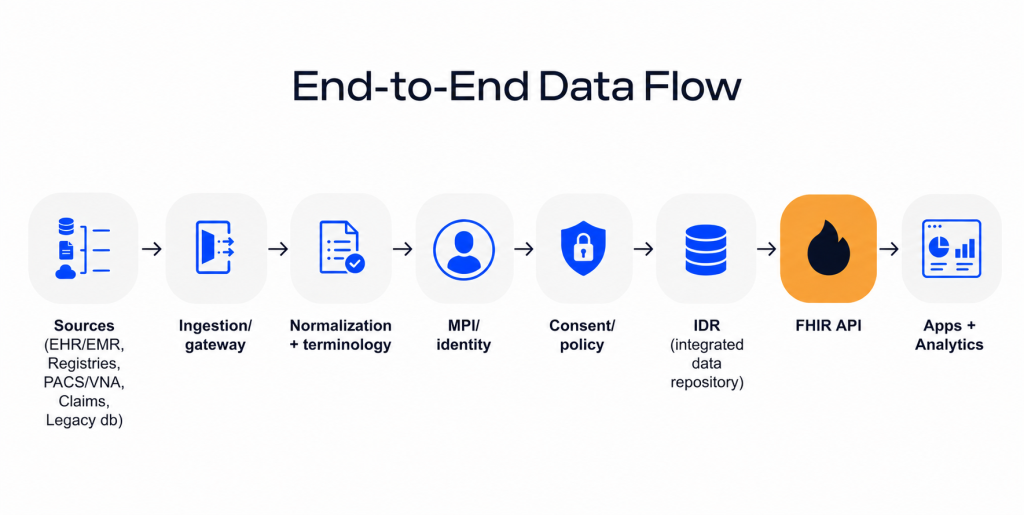
True exchange encompasses integration and accessible use of the data: ensuring that when information flows in, it is merged into longitudinal patient records, often via an integrated data layer that exposes standardized APIs (e.g., FHIR®) and supports downstream use. In other words, exchange should behave like an integrated data system where data is not just delivered, but made coherent and actionable.
In a modern HIE, “exchange” isn’t transport, it’s the ability to merge incoming fragments into a governed longitudinal record that can be queried, trusted, and safely reused across institutions.
It means harmonization of data — mapping local or unified codes and units into common standards so that, for example, a lab result from one system is meaningful in another.
It requires strong data governance and reliability measures: an HIE must deliver accurate, timely information consistently (e.g., 24×7 availability of results) and enforce policies on privacy, consent, and audit logging to maintain trust. When these controls are built into the architecture, the same data can support integrated data analysis rather than just “lookups”.
A successful HIE positions itself as an integrator and steward of shared health data — curating a usable community health record, managing identity and consent, and providing value-added tools like alerts and analytics — rather than just a conduit.
Modern exchange initiatives focus on data use and meaning (making sure exchanged data can be understood and used in care decisions) and on governance and trust (establishing rules so participants feel secure sharing data). Designing the IDR starts with understanding the repository types you must integrate.
Examples of Existing Health Repositories
Health data typically resides in multiple repository types that have different standards, latency, and privacy constraints:
EHR/EMR data stores: primary sources for encounters, notes, orders, and results; integration often requires vendor-specific mapping and interface work.
National or regional registries: immunizations, reportable labs, prescriptions, disease registries; valuable for population health but governed by jurisdictional access rules.
Document and image archives (PACS/VNA, scanned docs): imaging plus document-heavy content; useful, but harder to normalize into discrete data.
Claims and billing systems: claims-based history and eligibility; helpful for longitudinal views, but often batch-oriented and coded differently.
Successful integration starts with a thorough inventory of all sources in scope, plus clarity on sensitivity and ownership (for example, behavioral health data often has additional protections).
Why Legacy Health Repositories Become a Bottleneck
Many healthcare organizations already have repositories. The bottleneck emerges when those legacy assets are forced to operate as cross-organization infrastructure – without the interoperability, governance, and performance characteristics required by modern HIEs.
Siloed clinical data is the first pressure point: hospital-specific databases, lab and imaging silos, and payer/public health datasets were built around local workflows and contracts. The result is fragmented data systems where the same patient’s longitudinal story is partitioned by institution and vendor.
Non-standard data models are the second: custom schemas and HL7 v2-only “pipes” can move messages but still fail semantic interoperability. This is where you need deliberate modeling choices and a canonical strategy aligned to integration patterns.
Limited real-time capabilities become the third: batch exchange and weak API surfaces prevent event-enabled workflows (notifications, subscriptions, care coordination triggers). That limitation is often what forces modernization from “interfaces” to a modern repository and API design.
Finally, scaling and compliance requirements are different at HIE level. GDPR and HIPAA set expectations around protecting personal data / PHI and enforcing appropriate use and disclosure – which typically requires policy + technical controls such as least-privilege access, audit logging, and consent enforcement.
How a national program built an IDR-like clinical repository layer to store, normalize, and securely serve longitudinal records as part of a broader HIE ecosystem.
What Is an Integrated Health Data Repository in Modern HIE?
IDR is not just a larger database. In a modern HIE, it is the layer that collects, normalizes, and serves integrated data from multiple repositories so applications can query a consistent longitudinal record.
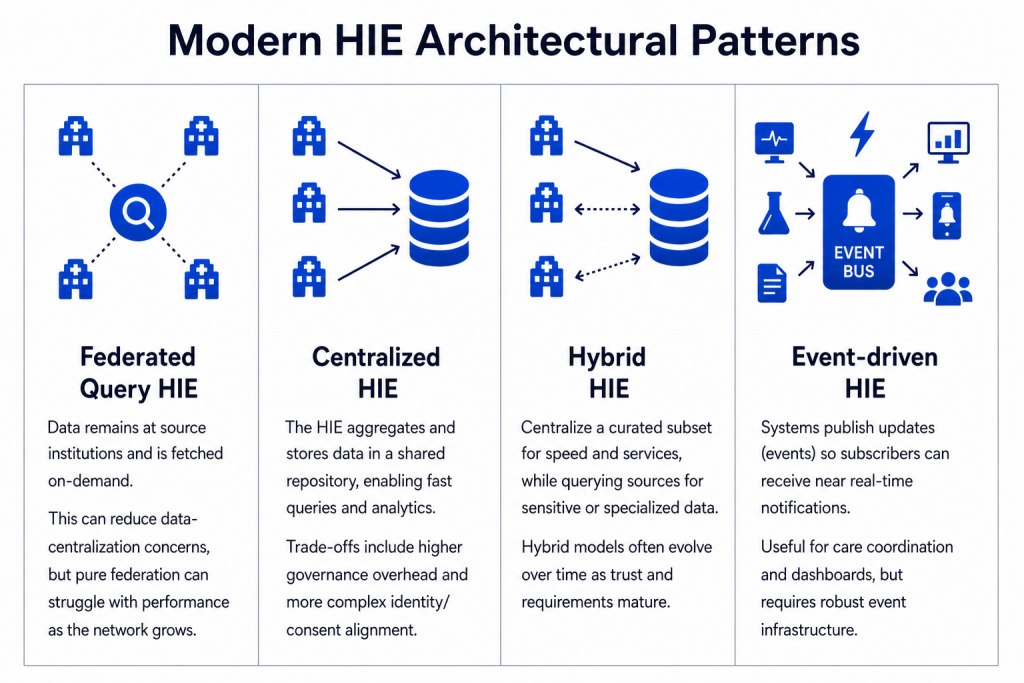
Depending on governance and stakeholder constraints, an IDR may be implemented as: a centralized data repository that receives feeds from participants, or a hybrid architecture where a curated subset is centralized while sensitive/specialized data remains federated.
When teams extend the IDR for analytics and reporting, it may also play the role of an integrated data warehouse (or even a national data warehouse in national-scale programs), enabling standardized queries, population health measures, and BI pipelines — i.e., integrated data analytics at scale.
In many HIE contexts, you will also see the term clinical data repository used for the clinical-facing “community record” store; the practical point is that the repository must be designed as a governed, interoperable service layer, not only storage.
FHIR-first design is central to this direction: Health Level Seven International defines FHIR as “a standard for exchanging healthcare information electronically.” This is why many teams treat the IDR as an “integrated data solutions” layer that normalizes inputs (HL7 v2, CDA, database extracts) and exposes a standards-based API surface (FHIR where feasible) to downstream apps and services.

Modern HIE Architectural Patterns for Legacy Integration
Over time, several HIE architecture models have emerged to integrate legacy systems. Most real-world ecosystems end up in a hybrid combination:
Integration Strategy: Step-by-Step Approach
Successfully integrating legacy data sources into an HIE requires a systematic strategy, because each step becomes a building block of the integrated repository outcome (canonical model, interoperability layer, MPI, governance, and API exposure).
Step 1: Inventory and Classify Data Sources
Begin with a comprehensive inventory of all existing data repositories and systems that will feed the HIE, because this defines the ingestion and normalization scope for a future centralized or hybrid IDR.
Catalog each source by type (EHR, lab system, registry, etc.), the data it holds, and sensitivity. This step also involves assessing the technical interfaces available and baseline data quality. A practical add-on here is to map each source to its likely landing role in the target architecture: feed for centralized data repository, federated endpoint, or candidate for IDR ingestion.
Step 2: Choose Data Exchange Primitives (Documents vs. Discrete Data)
Decide on the form(s) of data exchange the HIE will use with each source. Document-based exchange can be simpler initially, while discrete data exchange enables automation and queryability. This is also where many implementations decide whether the target is primarily an exchange network, or an IDR-centric data solutions platform that supports both exchange and integrated data analytics.
Many ecosystems still rely heavily on CDA and HL7 v2 while FHIR APIs are emerging. For example, a U.S. national survey of HIE organizations found widespread use of CDAs and HL7 v2, with a smaller share reporting HL7 FHIR API use.
Step 3: Normalize Semantics and Models
Implement a robust data normalization plan: map codes to standard vocabularies where possible, standardize units, and normalize structures. This is foundational so your integrated data system is not just connected, but comparable. Align this work to your canonical model and your IDR design choices; otherwise, you will build an integrated data repository that cannot support reliable data analysis.
Step 4: Identity Management and Record Linkage
Establish an enterprise Master Patient Index (MPI) or comparable identity strategy. Strong identity resolution is required for longitudinal views, consent enforcement, and trustworthy integrated data analytics.
Step 5: Consent, Privacy and Access Control
Develop a consent model and access control scheme from the outset, and integrate it into the system design. Modern HIEs also implement strong security measures like OAuth 2.0 and OpenID Connect for authentication/authorization patterns in API ecosystems: OAuth 2.0 is defined in an IETF standard, and OpenID Connect (from the OpenID Foundation) defines an identity layer on top of OAuth 2.0.
On the regulatory side, GDPR and HIPAA establish expectations and rules for protecting personal data/PHI and governing use/disclosure. For an applied view of controls in exchange environments, see HIE security standards.
Step 6: Data Quality and Observability
Treat data quality and system observability as first-class aspects of the integration. Monitor duplicates, missing fields, inconsistent mapping, and latency. This is where integrated repositories become trusted enough for clinical use and for integrated data analytics programs.
Need a phased plan before you integrate?
We are here to help. Check our
Healthcare Interoperability solution developmentCommon Mistakes in Repository Modernization
Treating it as a simple data migration. If you only “move data,” you preserve fragmentation. Modernization must include interoperability architecture (identity, consent, normalization, API design) so the repository system becomes a functioning integrated data system rather than a new silo.
Skipping data standardization. “Garbage-in, garbage-out” is amplified in HIE programs: without canonical models and vocabulary alignment, the IDR cannot support reliable integrated data analytics.
Over-centralization. A centralized data repository can be the right choice, but ignoring hybrid/federated patterns can increase political, privacy, and operational risk. An IDR often works best as a selectively centralized, governed layer (and in analytics contexts, an integrated data warehouse) rather than a “store everything centrally” default.
Underestimating governance and security. Consent enforcement, audit, privacy, and security controls must be designed in, not bolted on.
How Edenlab Supports Repository Integration Projects
Edenlab supports repository modernization programs that aim to turn fragmented legacy repositories into integrated data solutions that can scale.
Architecture design and audit: legacy assessment, target architecture, and phased roadmap, typically starting with interoperability gaps and governance foundations.
Implementation and integration delivery: building the interoperability layer to ingest and normalize data, integrate and store information in a governed repository, and expose standardized APIs.
FHIR-based transformation for legacy feeds: where systems still emit HL7 v2 messages, they can be mapped into FHIR-based representations for downstream use.
Analytics enablement: designing the integrated data warehouse / reporting layer so integrated data analytics can run reliably across sources.
Conclusion
Replacement is not the only path. Integration is often safer, faster, and more strategic: evolve legacy repositories into an IDR-centric integrated data repository that supports interoperability, governance, and performance. When designed as an integrated data system (not just storage), the repository layer can also serve as a clinical data repository for longitudinal care views and as an integrated data warehouse for integrated data analytics and reporting.

Modernize repositories without a risky rebuild
Tell us what repositories you have today (EHRs, registries, PACS/VNA, claims, legacy databases) and what constraints you’re under. We’ll help shape a phased roadmap.
FAQs
Can legacy HL7 v2 systems be integrated into a FHIR-based architecture?
Yes. A common approach is to keep HL7 v2 feeds at the edge and transform them into FHIR resources in the interoperability layer (HL7 provides V2-to-FHIR mapping guidance), so downstream services consume data through a consistent FHIR-first API surface.
What makes Edenlab’s approach to HIE modernization different from other vendors?
The emphasis is incremental modernization: define target architecture and governance early, deliver value in phases (connect, normalize, expose APIs, harden governance), and avoid risky “rip-and-replace” while still moving toward an IDR-centric integrated data repository.
How does Edenlab ensure compliance with GDPR/HIPAA when integrating legacy data?
By engineering compliance controls into the architecture: consent enforcement, least-privilege access, authentication/authorization, audit logging, data minimization, and security monitoring aligned to regulatory obligations.
Can Edenlab integrate both hospital-level and regional/national-level repositories?
Yes. The patterns (hybrid/centralized/federated) can be applied at multiple scales, and Edenlab references national-level work in its public case studies, which is useful as an architectural benchmark.
Read how we built a National E-Health System where the same interoperability, governance, identity, and consent patterns were applied at country scale: 36.5M+ patient records, 33 regional EHRs integrated, 8,275+ facilities, 15,000+ pharmacies, ~1,000 TPS current load, and 75M digital prescriptions issued.
How long does it take to transform existing health repositories into a fully integrated HIE-ready system?
It depends on source count, data quality, and governance readiness. Programs typically progress via phased delivery: an assessment and pilot integrations first, then onboarding waves until coverage, performance, and trust meet operational needs.
Stay in touch
Subscribe to get insights from FHIR experts, new case studies, articles and announcements
Great!
Our team we’ll be glad to share our expertise with you via email




